Cerebellitis as a Rare Manifestation of HSV Encephalitis: A Case Report
DOI:
https://doi.org/10.5195/ijms.2025.3131Keywords:
Herpes Simplex Encephalitis, Herpes Encephalitis, Herpetic Encephalitis, Herpes Simplex Virus 1, Cerebellar AtaxiaAbstract
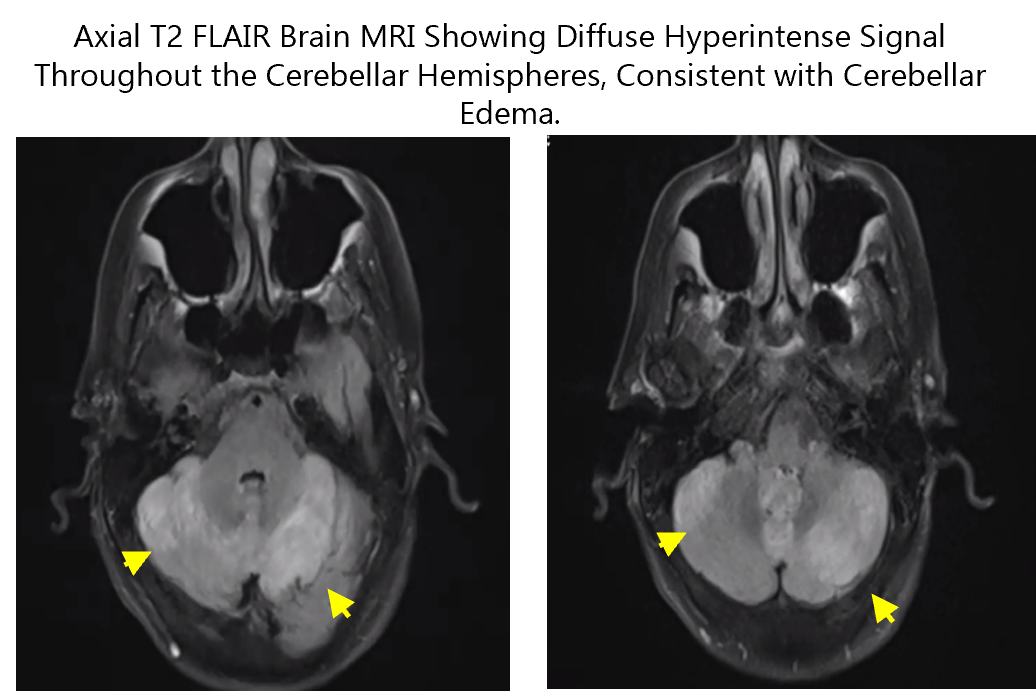
Background: Herpes Simplex Virus (HSV) is a common cause of encephalitis. A feared complication of HSV encephalitis is hemorrhage and necrosis of the brain parenchyma most commonly in the temporal lobe(s). Less common sites of focal necrosis include the insula and inferior frontal lobes. A rare presentation of HSV encephalitis is cerebellitis. Case: A 74-year-old female presented with a 1-month history of progressive balance difficulty and dizziness. The neurological exam showed truncal ataxia and scanning dysarthria. Serum labs were largely unremarkable, except for elevated sedimentation rate (ESR). Brain MRI revealed diffuse cerebellar swelling and T2 signal changes, with left medial enhancement. Cerebrospinal fluid (CSF) analysis showed elevated red blood cells (WBCs 5, RBCs 438, protein 54.7, glucose 64) and was positive for HSV-1 PCR. The CSF autoimmune encephalopathy panel was negative. She was treated with acyclovir 10 mg/kg every 8 hours for 14 days and IV methylprednisolone 1000 mg daily for 5 days, followed by an oral prednisone taper. Clinical improvement in ataxia and dizziness was observed soon after treatment began, with decreased cerebellar edema and enhancement on repeat MRI. After discharge, the patient was lost follow-up, and long-term neurological status remains unknown. Conclusions: Recognition of atypical HSV encephalitis is crucial as encephalitis has a broad differential and CSF HSV PCR is a widely available and highly specific test. Rapid administration of acyclovir is the current standard of care. An addition of pulse dose methylprednisolone may also impart symptomatic and radiographic benefit.
References
Armangué T, Olivé-Cirera G, Martínez-Hernández E, Rodés M, Peris-Sempere V, Guasp M, et al. Neurologic complications in herpes simplex encephalitis: clinical, immunological and genetic studies. Brain. 2023;146(10):4306–19.
Bradshaw MJ, Venkatesan A. Herpes simplex virus-1 encephalitis in adults: pathophysiology, diagnosis, and management. Neurotherapeutics. 2016;13(3):493–508.
Campos LG, Rossato R, Santos RP, Duarte JA, Vedolin L. Acute cerebellitis caused by herpes simplex virus. Clin Biomed Res. 2019;39(1):104–5.
Ciardi M, Giacchetti G, Fedele CG, Tenorio A, Brandi A, Libertone R, et al. Acute cerebellitis caused by herpes simplex virus type 1. Clin Infect Dis. 2003;36(3):e50–4.
Guerreiro Stucklin AS, Grotzer MA. Cerebellar tumors. Cerebellum Disord Treat. 2018;155:289–99.
Hodzic E, Hasbun R, Granillo A, Tröscher AR, Wagner H, Tim M, et al. Steroids for the treatment of viral encephalitis: a systematic literature review and meta-analysis. J Neurol. 2023;270:3603–15.
Jouan Y, Grammatico-Guillon L, Espitalier F, Cazals X, François P, Guillon A. Long-term outcome of severe herpes simplex encephalitis: a population-based observational study. Crit Care. 2015;19(1):1–9.
Kamei S. Evaluation of combination therapy using aciclovir and corticosteroid in adult patients with herpes simplex virus encephalitis. J Neurol Neurosurg Psychiatry. 2005;76(11):1544–9.
McKeon A. Purkinje cell cytoplasmic autoantibody type 1 accompaniments. Arch Neurol. 2011;68(10):1282.
Meyding-Lamadé U, Jacobi C, Martinez-Torres F, Lenhard T, Kress B, Kieser M, et al. The German trial on aciclovir and corticosteroids in herpes-simplex-virus-encephalitis (GACHE): a multicenter, randomized, double-blind, placebo-controlled trial. Neurol Res Pract. 2019;1(1):1–10.
Paketci C, Edem P, Okumus C, Sarioglu FC, Bayram E, Hiz S, et al. Herpes simplex virus-1 as a rare etiology of isolated acute cerebellitis: case report and literature review. J Neurovirol. 2019;26(2):270–2.
Pedroso JL, Vale TC, Braga-Neto P, Dutra LA, França MC Jr, Teive HAG, et al. Acute cerebellar ataxia: differential diagnosis and clinical approach. Arq Neuropsiquiatr. 2019;77(3):184–93.
Ramos-Estebanez C, Lizarraga KJ, Merenda A. A systematic review on the role of adjunctive corticosteroids in herpes simplex virus encephalitis: is timing critical for safety and efficacy? Antivir Ther. 2013;19(2):133–9.
Sawaishi Y, Takada G. Acute cerebellitis. Cerebellum. 2002;1(3):223–8.
Matthews E, Beckham JD, Piquet AL, Tyler KL, Chauhan L, Pastula DM. Herpesvirus-associated encephalitis: an update. Curr Trop Med Rep. 2022;9(3):92–100.
Published
How to Cite
License
Copyright (c) 2025 Cole Cimoch, Daniel Groblewski, David Mendoza

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors who publish with this journal agree to the following terms:
- The Author retains copyright in the Work, where the term “Work” shall include all digital objects that may result in subsequent electronic publication or distribution.
- Upon acceptance of the Work, the author shall grant to the Publisher the right of first publication of the Work.
- The Author shall grant to the Publisher and its agents the nonexclusive perpetual right and license to publish, archive, and make accessible the Work in whole or in part in all forms of media now or hereafter known under a Creative Commons Attribution 4.0 International License or its equivalent, which, for the avoidance of doubt, allows others to copy, distribute, and transmit the Work under the following conditions:
- Attribution—other users must attribute the Work in the manner specified by the author as indicated on the journal Web site; with the understanding that the above condition can be waived with permission from the Author and that where the Work or any of its elements is in the public domain under applicable law, that status is in no way affected by the license.
- The Author is able to enter into separate, additional contractual arrangements for the nonexclusive distribution of the journal's published version of the Work (e.g., post it to an institutional repository or publish it in a book), as long as there is provided in the document an acknowledgment of its initial publication in this journal.
- Authors are permitted and encouraged to post online a prepublication manuscript (but not the Publisher’s final formatted PDF version of the Work) in institutional repositories or on their Websites prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work. Any such posting made before acceptance and publication of the Work shall be updated upon publication to include a reference to the Publisher-assigned DOI (Digital Object Identifier) and a link to the online abstract for the final published Work in the Journal.
- Upon Publisher’s request, the Author agrees to furnish promptly to Publisher, at the Author’s own expense, written evidence of the permissions, licenses, and consents for use of third-party material included within the Work, except as determined by Publisher to be covered by the principles of Fair Use.
- The Author represents and warrants that:
- the Work is the Author’s original work;
- the Author has not transferred, and will not transfer, exclusive rights in the Work to any third party;
- the Work is not pending review or under consideration by another publisher;
- the Work has not previously been published;
- the Work contains no misrepresentation or infringement of the Work or property of other authors or third parties; and
- the Work contains no libel, invasion of privacy, or other unlawful matter.
- The Author agrees to indemnify and hold Publisher harmless from the Author’s breach of the representations and warranties contained in Paragraph 6 above, as well as any claim or proceeding relating to Publisher’s use and publication of any content contained in the Work, including third-party content.
Enforcement of copyright
The IJMS takes the protection of copyright very seriously.
If the IJMS discovers that you have used its copyright materials in contravention of the license above, the IJMS may bring legal proceedings against you seeking reparation and an injunction to stop you using those materials. You could also be ordered to pay legal costs.
If you become aware of any use of the IJMS' copyright materials that contravenes or may contravene the license above, please report this by email to contact@ijms.org
Infringing material
If you become aware of any material on the website that you believe infringes your or any other person's copyright, please report this by email to contact@ijms.org